

Authors
|
|||||||
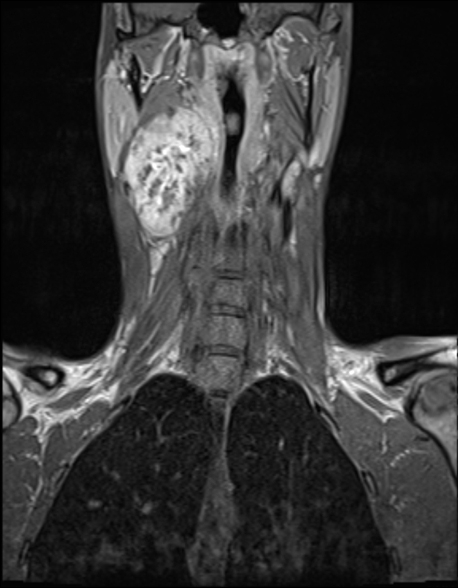
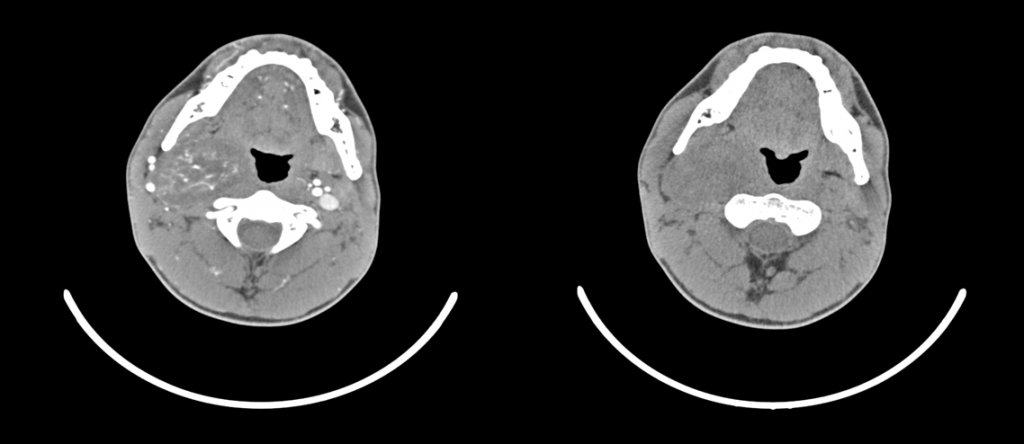
AbstractSchwannoma is a rare tumor arising from the peripheral nerve sheath. Ancient schwannoma is a rare, slow-growing variant. In this report we presented a rare case with ancient schwannoma of symphatetic nerves of the neck which caused postoperative Horner Syndrome. To our knowledge, there is only a few reports about ancient schwannoma of sympatetic nerves in English literature. Because of possible complications of surgery of schwannomas such as Horner Syndrome, it must be kept in mind in the differential diagnosis of lateral neck masses.IntroductionSchwannoma is a rare tumor arising from the peripheral nerve sheath. It frequently occurs in the head and neck region and the extremities. Schwannomas in the head and neck region generally derive from the cervical sympathetic nerve and the nervus vagus[1]. Ancient schwannoma is a rare, slow-growing variant. The term ‘ancient’ was first used by Ackerman and Taylor to indicate the prolonged course of degenerative changes in the appearance of this entities [2]. It generally occurs as a slow-growing, painless, benign mass in the neck [3]. Malign transformation may be seen together with Von Recklinghausen disease[4]. In some advanced cases, symptoms such as cough, dysphagia, cranial nerve paralyses, Horner’s syndrome and hearing loss may result from pressure on surrounding structures. In this report we presented a rare case with ancient schwannoma of symphatetic nerves of the neck which caused postoperative Horner Syndrome [5]. [ ]To our knowledge, there is only a few reports about ancient schwannoma of sympatetic nerves in English literature. Case ReportA 17-year-old male presented to our clinic with a painless swelling in the upper right part of the neck existing for approximately two years. Otorhinolaryngological examination revealed a well-marginated, pulsatile mass, 6.5 cmin size, beneath the right corner of the mandible. The pharynx was displaced medially. Ultrasonography was performed which revealed a heterogenic hypoechoic mass differentiated from surrounding tissue with good margins containing cystic areas, 9x5 cm in size, neighboring on the carotid. A mass well differentiated from heterogeneously contrasting surrounding tissue was observed on post-contrast images at computerized tomography (CT) of the neck.
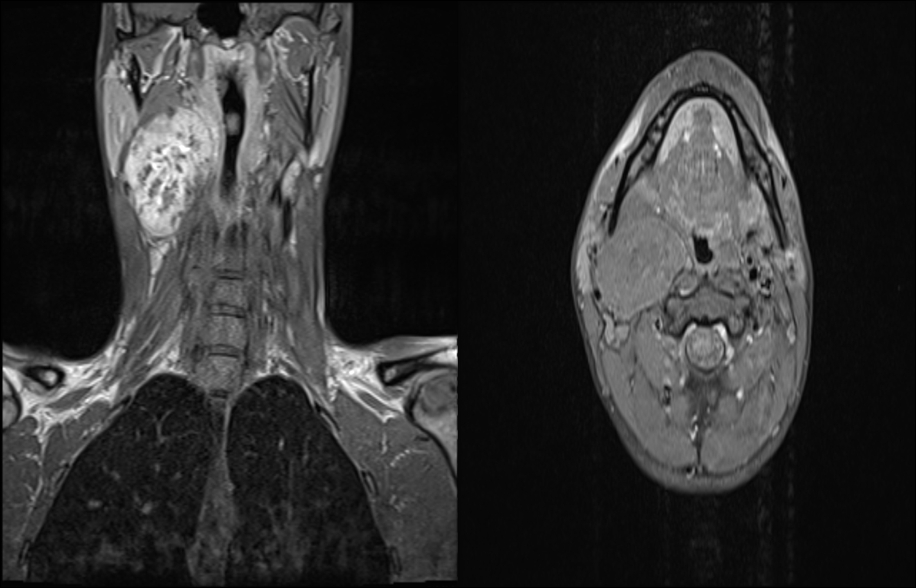
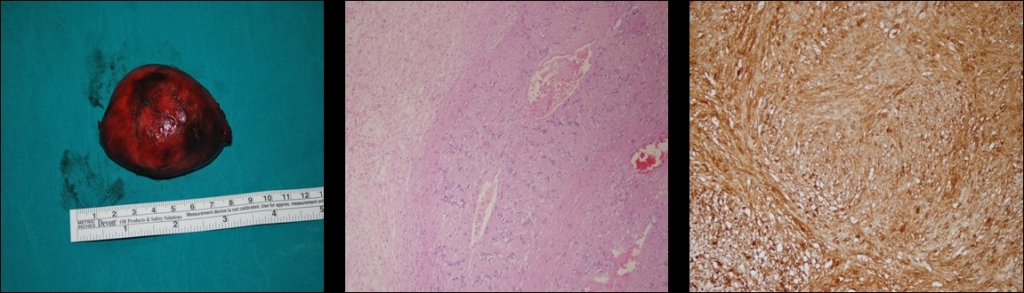
DiscussionSchwannomas are benign, encapsulated tumors deriving from Schwann cells in the peripheral nerve sheath. Schwannomas are typically solitary, encapsulated tumors gradually extending outside the fibrils from which they originate. Histopathologically, they consist of varying proportions of Antoni-A and Antoni-B cell patterns. Antoni-A areas consist of palisading sequences of compact spindle-shaped cells, while Antoni-B areas are loose hypocellular regions. Necrosis and cystic degeneration, hyalinization and calcification may be seen in the stroma[6]. In histological terms, five schwannoma variants have been described; common, plexiform, cellular, epithelioid, and ancient schwannomas [7]. The term ancient is used in order to describe the tumor’s gradual degenerative changes, diffuse hypocellular areas, nuclear hyperchromasia and pronounced nuclear atypia [3]. Schwannomas are found in the lateral region of the neck. They constitute encapsulated tumors that are horizontally mobile but vertically immobile and that may sometimes lead to displacement in the lateral pharyngeal wall[8]. Ancient schwannomas are rare and particularly prevalent in elderly subjects[6]. They generally emerge in the 3[rd] and 4[th] decades, as slow-growing, painless masses. They may cause symptoms through the pressure they place on surrounding tissues[9]. In some advanced cases this pressure on neighboring tissues may result in symptoms such as cough, dysphagia, cranial nerve paralyses, Horner’s syndrome and loss of hearing [10]. Radiological findings in ancient schwannomas are similar to those in other schwannomas. At ultrasonography they appear as hypoechoic masses with regular margins, and calcifications may be determined. CT and MRI can assist with the diagnosis of schwannoma. At contrast enhanced CT they appear as a mass differentiated with well-defined margins from heterogeneously contrasting surrounding tissues. Isobe et al. suggested that MRI is of greater usefulness. Schwannoma is generally hypointense on T1 weighted MRI images and hyperintense on T2 weighted images [11]. Schwannomas are radioresistant tumors. Treatment essentially consists of surgery. In terms of surgical technique, the ideal approach is dissection with protection of the nerve. Total excision was performed in our case, with a transcervical approach. The mass was dissected from surrounding tissues and the neurovascular bundle[12]. After excision, permanent or gradually resolving sequelae such as Horner’s syndrome may persist [13]. Postoperative Horner’s syndrome developed in our case. However, this resolved during 4-month follow-up. Conclusion Ancient schwannoma of cervical sympathetic chain is very rare disease with only a few reports in English literature. Because of possible complications of surgery of schwannomas such as Horner Syndrome, it must be kept in mind in the differential diagnosis of lateral neck masses. References
|
|||||||
| Keywords : Ancient Schwannoma , Ansa Servikalis , Horner Sendromu | |||||||
|