

Authors
|
|||||
AbstractLateral sinus thrombosis (LST) is a rare complication of middle ear diseases: It is usually related to acute or chronic otitis media. Its mortality was higher in the pre-antibiotic era.The Authors report a case of a 12-year-old girl who had lateral sinus thrombosis and otitic hydrocephalus contributory acute otitis media with a 3 weeks history complicating to thrombosis. According to the etiological workup, she had a mutation in the heterozygote methylenetetrahydrofolate reductase gene. Based on this case, the clinical approach of the disease and related literature are described. At the present time, LST in children is considered an unusual complication of acute otitis media. For diagnosis suspicion and imaging is essential. IntroductionLateral sinus thrombosis (LST) is a well-known intracranial complication of acute or chronic otitis media. Before the antibiotic era, the mortality rate was reached up to 100%.The incidence of LST has decreased due to the wide-spread usage of antibiotics [1]. LST usually develops as a complication of chronic otitis media caused by erosion of neighboring bone by cholesteatoma or as a complication of acute otitis media (AOM) by thrombophlebitic dissemination through the emissary vein in the intact bone [2, 3]. After dissemination of infection to lateral sinus, adherence of fibrin, blood cells and platelets can form a mural thrombus. Finally, an increase in thrombus volume may result in obliteration of lateral sinus. Especially in young adults, LST is frequently seen in association with inherited (AT III, protein C or Protein S deficiency, Factor V Leiden mutation, MTFR gene mutation, prothrombin gene 20210A mutation) or acquired (neoplasia, trauma, autoimmune diseases, neurosurgical procedures, myeloproliferative diseases, antiphospholipid syndrome, pregnancy or oral contraceptives) hypercoagulable state [2,3]. The methylenetetrahydrofolate reductase (MTHFR) gene mutation causes elevated homocysteine levels which eventuate an increased risk of atherosclerosis, heart attack, stroke, and venous thrombosis. The patients with MTHFR gene mutation usually have high levels of serum homocysteine [4]. In this paper, we present a case of a 12-year-old girl suffered from otitis media with lateral sinus thrombosis which is related to MTHFR gene mutation. Case Report12 years old female patient has admitted to our emergency department with a headache persisted over a week and blurred vision and diplopia for three days. She had a history of otitis media which was treated with antibiotics 20 days ago. The neuro-otologic evaluation revealed left sixth cranial nerve palsy, bilateral papilledema, the amber-gold color of the left eardrum (Figure 1).
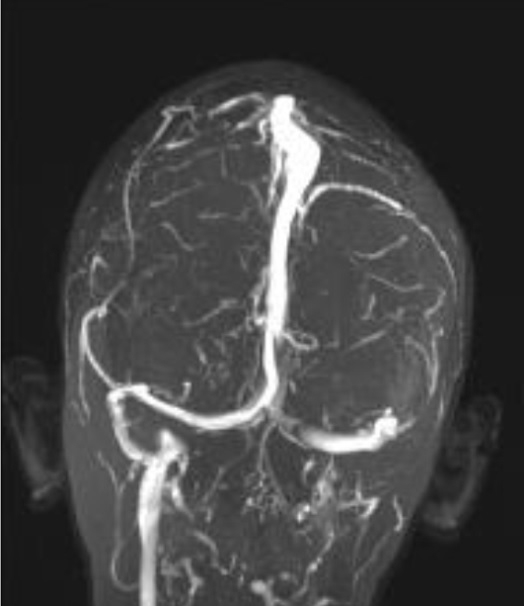
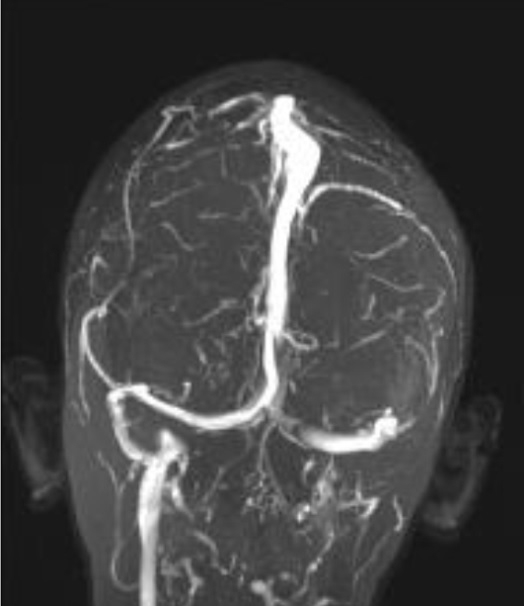
She had no fever (36.5 °C). There was no post-auricular hyperemia or edema or other cranial nerve pathologies. We immediately performed cranial magnetic resonance (MR) imaging and temporal bone computed tomography (CT) scan without contrast in the emergency unit. Magnetic resonance imaging revealed suspicion of left LST. Computed tomography scan showed effusion but no coalescent in the mastoid cells. Subsequently, MR venography images were taken to confirm the diagnosis. The lateral sinus and the jugular vein were nearly totally occluded in MR venography (Figure 2).
After hospitalization left myringotomy was performed under local anesthesia but there was no effusion in the middle ear space. The white blood cell count and CRP level were in normal range. After the diagnosis of LST contributing to otitic hydrocephalus, parenterally ceftriaxone 2x1 gr i.v., acetazolamide 250mg 2x1 p.o. and clexane 0.4ml 2x1 subcutaneously per /day were started. An etiological workup revealed heterozygote MTHFR gene mutation. There were no other abnormalities in prothrombic disposition tests. The recanalization of lateral sinus and the jugular vein were seen in the control MR venography which was performed one week after the diagnosis. The patient completely recovered. Low molecular weight heparin (0.4ml/day) treatment was prescribed for three months due to the suggestion of the pediatric hematology department. DiscussionLateral sinus thrombosis can be classified as non-septic or septic LST. Etiologies of these conditions are different. Non-septic LST is not associated with ear infections. However septic LST is seen as a complication of head and neck infection [1]. In septic LST specifically severe headache, otalgia, picket-fence fever and papilloedema are the most frequent presenting symptoms and signs Tenderness and edema over mastoid (Griesinger sign) are pathognomonic for septic LST [5]. In our case, the patient didn’t have fever, tenderness and edema over mastoid. However she had headache, papilloedema and diplopia due to sixth cranial nerve palsy and she had a history of AOM.The unusual admission of our patient might be due to her antibiotic usage for AOM. The clinical presentation of otogenic LST as a complication of AOM can be masked by antibiotic treatment. Vomiting, headache, visual impairment complaints and a history of AOM are seem to be indicative of the diagnosis of otitic hydrocephalus. MRIs of patients with these symptoms should be carefully investigated to make an early diagnosis of LST with increased intracranial pressure [6]. The bacteriological investigation was discussed in different studies. In the studies reporting bacterial analysis, the culture was positive in 54 out of 100 children (54%), with streptococci being the most frequent group in 30 (56%) [7]. The thrombotic activity of streptococci has been described in clinical cases and studied in animals, but has not been completely elucidated. However, in a substantial number of patients, up to 45%, cultures yielded negative results. Thus, the true frequency and the impact of the various bacteria remain unknown [7]. In our patient, there was no otorrhea.or discharge after myringotomy. Therefore, bacteriologic cultures could not be performed. When there is a clinical suspicion of ICCs during a middle ear infection, imaging is essential for diagnosis and treatment planning. Contrast-enhanced CT imaging of the brain and temporal bones reveal the sinus plate erosion and may show the “delta sign” (central non-enhancing clot surrounded by enhancing dural sinus wall), indicating sinus thrombosis and other ICCs, such as brain abscess and empyema [5]. In the diagnosis of LST, it is considered that MRI is superior to CT owing to its ability to show low or absent flow in the venous sinuses, clot formation and the presence of inflammation in the brain and meninges [1]. In MRI, a thrombus appears as increased signal intensity on T1 and T2 images. In MR venography, the absent signal of a transverse sinus is observed. However, this finding does not differentiate an atretic sinus from occluded sinus. In this case, in emergency unit, initially CT and MRI were performed without contrast injection. Therefore, for the exact diagnosis was confirmed by MR venography. When Novoa et al. [7] reviewed the literature for thrombophilia screening, in 5 studies, including their study ratios of prothrombin dispositions were calculated. There was a total of 39 patients and abnormal results were reported only in 9 children (23%). Four of these were found to be heterozygote for the C677T polymorphism in the MTHFR gene, one with an additional heterozygosity for factor V Leiden mutation. Four showed elevated markers of antiphospholipid syndrome. The remaining child had heterozygosity for factor V Leiden mutation [7]. Methylenetetrahydrofolate reductase gene mutation is involved in the metabolism of homocysteine and may account for reduced enzyme activity and elevated plasma homocysteine levels [8]. Although the exact mechanism of atherosclerosis and thrombosis is not clear, endothelial dysfunction, damage to endothelial cells and inflammation of blood vessels caused by reactive oxygen species are thought to be responsible for these diseases [9]. Severe hyperhomocysteinemia is rare, about 5%-7% of the total population is known to have mild hyperhomocysteinemia. The frequency of heterozygosity and homozygosity for MTHFR gene mutation in Turkish populations is 47.4% and 9.6%, respectively [10]. Most Authors agree that, in children, surgical treatment of septic LST combined with i.v. antibiotic therapy is standard. While mastoidectomy is performed in patients with AOM, radical or modified mastoidectomy is recommended in cases of cholesteatoma [1, 2, 5]. The role of anti-coagulation treatment in septic LST is still debatable [2]. If there is a coagulation disorder, anti-coagulation therapy is mandatory. Bradley et al. emphasized that the risk of complications related to LST (such as embolization and persistent sepsis) are balanced with the possible complications associated with anti-coagulation, especially within the pediatric population (such as thrombocytopenia, drug interactions, bleeding, hemorrhagic skin necrosis and bleeding) [2]. Interestingly, in our case, after antibiotic and anti-coagulation therapy, the sinus totally recanalized without the need of mastoidectomy. Conclusion: LST is considered as an unusual complication of otitis media requiring early accurate recognition and treatment. Clinic suspicion and imaging are essential to make a diagnosis and for planning strategy. Management of LST is controversial but usually consists of conservative surgical treatment combined with iv antibiotic therapy. However, in hypercoagulability states, anti-coagulant treatment is mandatory. References
Presented at01 – 04 Mayıs 2014 III. Ulusal Otoloji Nörootoloji Kongresinde [PP-36] nolu poster olarak sunulmuştur. |
|||||
| Keywords : Otitis media , lateral sinüs trombozu , Metilentetrahidrofolat redüktaz gen mutasyonu | |||||

|