

Authors
|
|||||||||||||
AbstractBackground: İntramasseteric hemangiomas (IMH) are seen very rarely and typically present as localized rubbery lumps at second or third decade. The main treatment is surgical exicion. Various surgical approaches have been reported such as intraoral approach, superficial parotidectomy approach, submandibular approach in the treatment of intramasseteric hemangioma. We presented our surgical approuch to intramasseteric mass in a pateint who attented our clinic with preauricular pain and swelling in this article.Case Report: fifty four years-old female patient described that the size of the swelling below her cheekbone has fluctuated over time. Physical examination showed a soft, painful 2-3 cm mass at right preauricular region. We successfully treated the lesion localized in deep of masseter muscle with modified Blair incision approach without doing superficial parotidectomy. Conclusion: IMH diagnosis is hard to establish due to scarcity of the disease. Swelling overlying masseter muscle should be investigated for IMH. Modified Blair incision approach without parotidectomy became safe and cosmetically favorable in presented patient. IntroductionIntramuscular hemangiomas (IMH) constitute 1% of benign skeletal muscle tumors. Fifteen percent of hemangiomas are seen in head and neck region, masseter and trapezius muscles being the most commonly affected muscles (60% among head and neck muscles). Other possible muscles include; periorbital muscles, sternocleidomastoid, temporal, geniohyoid and medial pterygoid muscles [1]. They typically present as localized rubbery lumps at second or third decade. Although there is no gender difference for IMHs overall, masseter hemangioma is more commonly seen in men [2]. Symptoms such as vibration, murmur, change in skin color are not detected. IMHs are accepted as congenital hamartomatous neoplasms that are not noticed until they abruptly grow, cause pain and cosmetic defect. It is suggested that hormonal and traumatic factors have a major role in the etiology of the disease and growth of the mass [3]. Histologically IMHs are classified as capillary (vessel diameter <140 μm), cavernous (vessel diameter > 140 μm), or mixed [4]. Treatment of choice for masseter IMH is surgical excision since it generates cosmetic defect and is painful. Different surgical approaches have been described for IMHs: for instance submandibular incision, intraoral incision, and approach with superficial parotidectomy [1-5]. This case report describes successful management of IMH adopting Blair Incision without superficial parotidectomy. Case Report54 year-old female presented to our otolaryngology Outpatient Clinic with swelling on right side of her face. She described that the size of the swelling below her cheekbone has fluctuated over time. She added that for the last 1 month there has been no change in size and she started feeling pain over her forehead, chin and ear. Physical examination showed a soft, painful 2-3 cm mass at right preauricular region (figure 1).
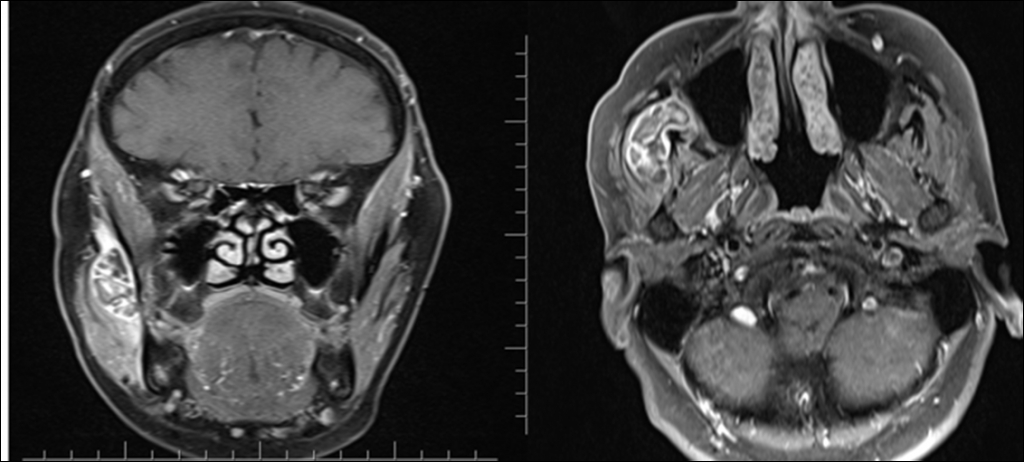
There were no abnormalities on laboratory tests. Patient’s medical and surgical history was relevant for myomectomy and lumbar discectomy operations. Magnetic Resonance Imaging (MRI) showed a 2.8x1.7 cm heterogeneous lesion with hemorrhagic component in right masseter muscle localized between mandibular and zygomatic arc showing contrast enhancement with intravenous contrast material (figure 2).
Fine needle aspiration biopsy was performed; cytology showed ‘fibrous tissue and blood elements’. Mass was excised under general anesthesia. Blair incision with external approach was performed without doing superficial parotidectomy. Skin and subcutaneous tissues were elevated to reach masseter muscle. Zygomatic and buccal branches of the facial nerve emerge from the parotid and diverge forwards lying over the masseter muscle. Masseter muscle dissection was made from the nerve-free area and mass was visualized. (figure 3).
Mass is totally excised by dissections made through ramus of mandibular at the posterior, maxillary bone medially and masseter muscle laterally (figure 4).
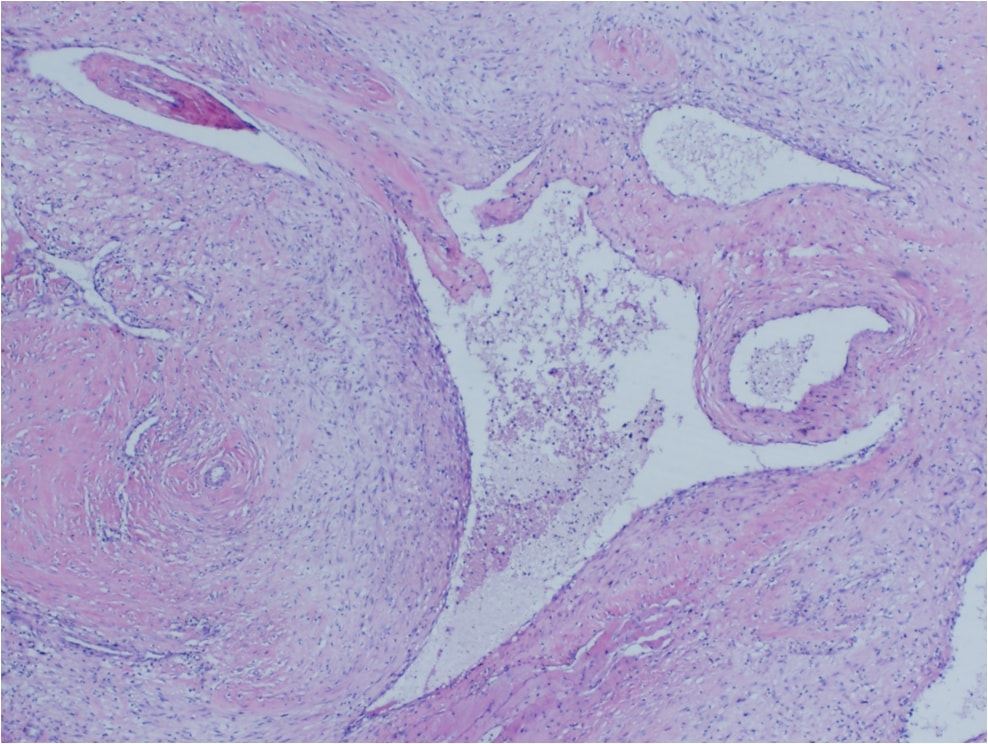
Facial nerve functions were intact after completion of the surgery. Pathologic examination of the specimen established the diagnosis as arteriovenous hemangioma (figure 5).
DiscussionIMH is a rarely encountered pathology. Rarity and insidious course of the disease with no typical presentation makes the diagnosis hard to determine. Most of the times it remains undiagnosed until surgery [3]. While making differential diagnosis of IMH; muscle hypertrophy, lymphadenopathy, lymphoma, schwannoma, diseases of the parotid gland, lymphangioma should be considered [1]. The initial imaging modality preferred for head and neck lumps is ultrasonography (USG) but it does not provide any specific finding for IMHs. Detection of vascular formations in and around the muscle with Doppler sonography can be helpful [7]. MRI is convenient for determining size and borders of the mas. Hemangiomas charactheristically enhance more on T2 weighted images compared to T1. FNAB is not diagnostic but presence of blood elements can support the diagnosis [4]. FNAB and MRI raised suspicion for IMH in present case but the definitive diagnosis could only be made after pathologic examination. Performing angiography and embolization before the surgery reduces risk of intraoperative bleeding [8]. While there are a number of treatment options for IMH such as sclerotherapy, cryotherapy, radiotherapy, steroid therapy and embolization; surgical excision is the treatment of choice [6]. Different surgical approaches have been proposed for IMH. Although intraoral approach is more advantageous in terms of better cosmetic results, risk of damaging zygomatic and buccal branches of facial nerve is higher. Approach with submandibular incision has also been proposed [1]. This latter technique is a better choice for lesions located inferiorly in masseter muscle since it is not possible to access superior and deeper lesions using submandibular incision. Another technique reported for IMH excision is superficial parotidectomy [9]. Even if facial nerve stays undamaged, doing superficial parotidectomy is unfavorable for the patient. The surgical technique carried out for this case is Modified Blair incision. Modified Blair incision is not only cosmetically favorable but also patient’s parotid gland is preserved which makes it more advantageous than other approaches (figure 6).
It should be pointed out that dissection should be meticulously carried out in order not to damage zygomatic and buccal branches of facial nerve while performing modified blair approach. Local recurrence rates have been reported between 9-28% [6]. IMH diagnosis is hard to establish due to scarcity of the disease. Swelling overlying masseter muscle should be investigated for IMH. Modified Blair incision without parotidectomy is a safe and cosmetically favorable surgical technique for treating IMH. References
Presented at37 Turkish National Congress of Otorhinolaryngology- Head and Neck Surgery, 28 October and 1 November 2015 |
|||||||||||||
| Keywords : hemanjiom , masseter kası , modifiye blair insizyonu | |||||||||||||





|