

Authors
|
|||||||
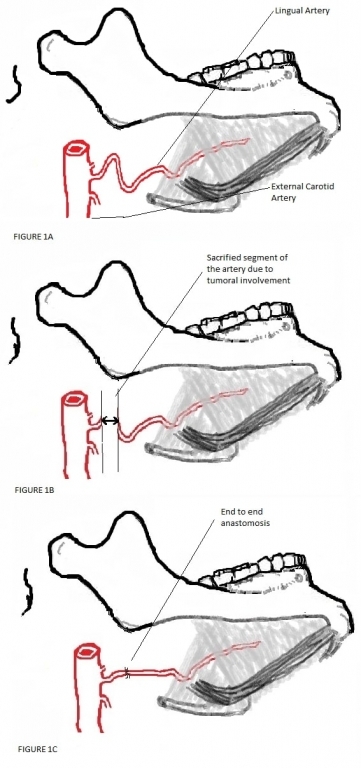
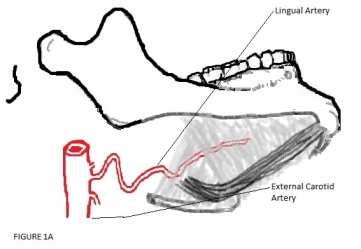
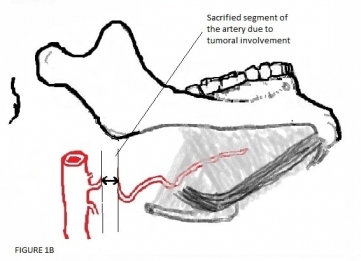
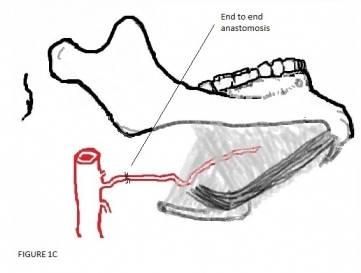
AbstractReconstruction of the tongue remains one of the most challenging conditions in head and neck oncology. Preserving the tongue is superior to any kind of reconstruction. In appropriate cases microsurgical revascularization is an eligible option for this purpose. In this paper we present a case in which both lingual arteries sectioned due to malignant tumor surgery and successfully revascularizated microsurgically on the right side. The patient had an uneventful recovery and the tongue remained viable in the follow-up period.IntroductionPreserving the tongue and its functions is essential for a good quality of life [1-2]. In tumor surgery, sacrification of both lingual arteries surgically is defined as unresectable, due to causing tongue necrosis. Revascularization of the tongue with micro vascular techniques is efficacious in selected cases where the blood supply to this organ is interrupted [3]. In the literature, there are few reports of such reconstruction. In this paper we describe a case, successfully revascularizated microsurgically of the right lingual artery, following a surgical resection for a recurrent laryngeal carcinoma ascending up to the base of the tongue. Case ReportA 63-year-old man presented with T3N2M0 squamous cell carcinoma of the supraglottic larynx was admitted with complaints of hoarseness, swallowing disorders and aspiration problems. He was treated with primary chemo-radiation therapy. He applied one year later with a recurrence swelling, predominantly involving the left side of the tongue base with extension to left ary-epiglottic fold, the left side of the epiglottis and the larynx. The vocal cords on both sides were free of tumor. There was no evidence of pathologic lymphadenopathy or distant metastasis in the PET/CT-scan and MRI of the neck. Biopsy indicated a recurrent squamous cell carcinoma. The patient underwent a total laryngectomy, partial pharyngectomy and resection of the tumor involving the base of the tongue. As expected, the left lingual artery and hypoglossal nerve was found to be surrounded by the tumor at surgery. Both of them had to be sectioned during dissection. At surgery we noticed that the right lingual artery was adherent to the tumor, but the artery was not invaded by it. We had to cut the right lingual artery from 10 milimeter distal to the external carotid artery during dissection for clear surgical margins. After completion of all laryngectomy and tumor resection, the proximal and distal stumps of the right lingual artery connected with a micro anastomosis technique (Figure 1: A-B-C).
The voluted structure of the lingual artery allowed an anastomosis in this way. Following the anastomosis, the blood flow was observed. Thereafter, a pectoralis major flap (PM-flap) prepared. A skin island of the PM flap is attached to the remainder hypo pharynx and the base of the tongue for reconstruction. The patient had an uneventful recovery and the tongue remained viable in the follow-up period. DiscussionResection of the tongue is commonly performed due to malignant head and neck tumors. Reconstruction of this organ following surgical resection remains one of the most challenging conditions in head and neck oncology. Recent trends in tongue reconstruction have focused on optimizing its functions and maximizing the quality of life [4]. Despite several reconstructive techniques can restore the shape, and the volume of the tongue quite well, but their functional outcomes are still limited [5]. The tongue plays a critical role in speech, swallowing, taste, oral hygiene and airway protection. It must be preserved as much as possible and avoided an unnecessary resection. Preservation its function is important to maintain a good quality of life [1-2]. The blood supply of the tongue is derived from the lingual arteries. It originates from the external carotid artery and courses on the deep surface of the hyoglossus muscle. The deep lingual artery then branches into a dorsal lingual artery and the sublingual artery. The veins form venae comitantes and join into the facial vein or the internal jugular vein. Its neural stimulus comes from the hypoglossal nerve [2,6]. In the case we reported, the tumor put at risk of the arterial flow of the tongue. On the left side, a large segment of the lingual artery and the left hypoglossal nerve was surrounded by the tumor, resulted in both sectioned. On the right side, following a resection of 1 centimeter segment of the lingual artery, end to end anastomosis was performed successfully due to its voluted formation; otherwise, an interposition graft had to be required (Figure 1 A), [7]. The tongue has also an extensive arterial network between its right and left side; hence, one sided revascularization was enough to supply the entire tongue. In this way, we avoided the need to a flap reconstruction. This case represents one of the few reports of a successfully resulted micro vascular revascularization of the tongue achieved by end-to-end anastomosis between the lingual artery remnants, after a tumor resection. There have been only 3 other reports of revascularization of the tongue secondary to tumor surgery in English literature. A single case of direct anastomosis of the lingual to the facial artery following tongue base cancer resection was reported by Shemen et al. [3] in 1988. Three cases reported by Thoma et al. [7] in 2001. They used interposition vein grafts in one patient successfully. In the other two patients, they did a direct anastomosis between the lingual artery remnants similar to our case, but one of them resulted with failure. One year later in 2002, Cole and Evans [8] reported a radial forearm free flap technique for both reconstruct the oropharingeal defect and restore the blood flow of the tongue as a bridge. The proximal end of the radial artery was anastomosed to the left external carotid artery, and the distal end anastomosed to the right lingual artery resulted in a successful perfusion. Additionally, in 1998 Buntic and Buncke [1] and in 2006 Egozi et al. [2] reported 2 cases microsurgically replanted successfully after a total, and a near total traumatic tongue amputation. In conclusion; tongue should be preserved as much as possible due to its crucial importance. Preserving the tongue is superior to any kind of reconstruction. In appropriate cases, microsurgical revascularization is an eligible option for this purpose. References
|
|||||||
| Keywords : Dil , tümör , lingual arter , revaskülarizasyon | |||||||
|