

|
|||||||||
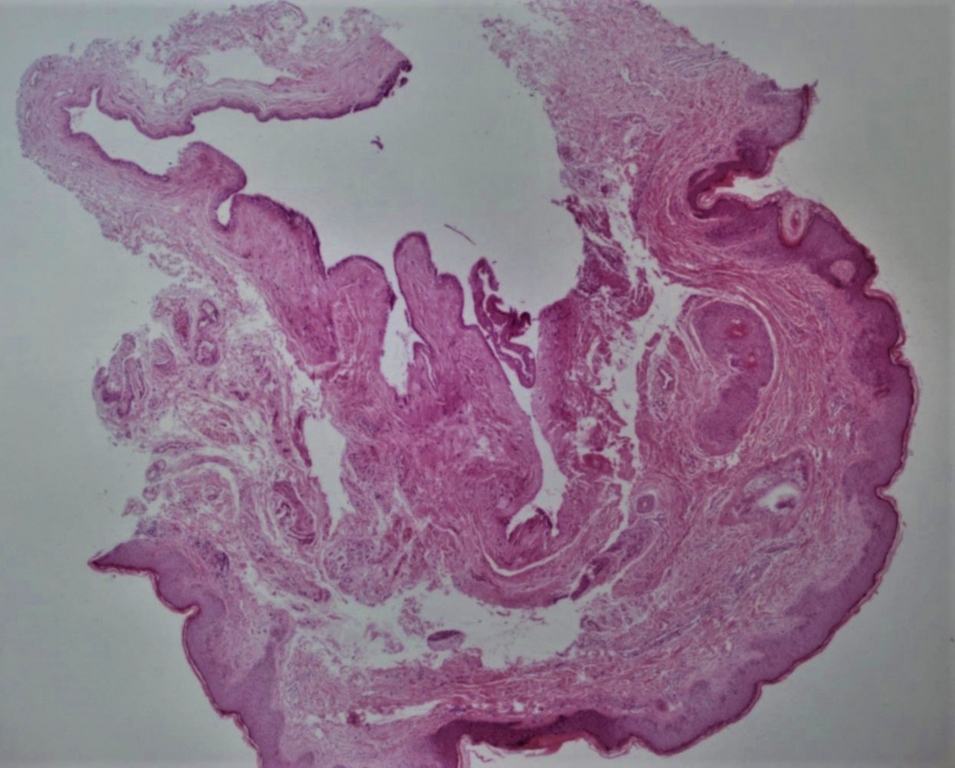
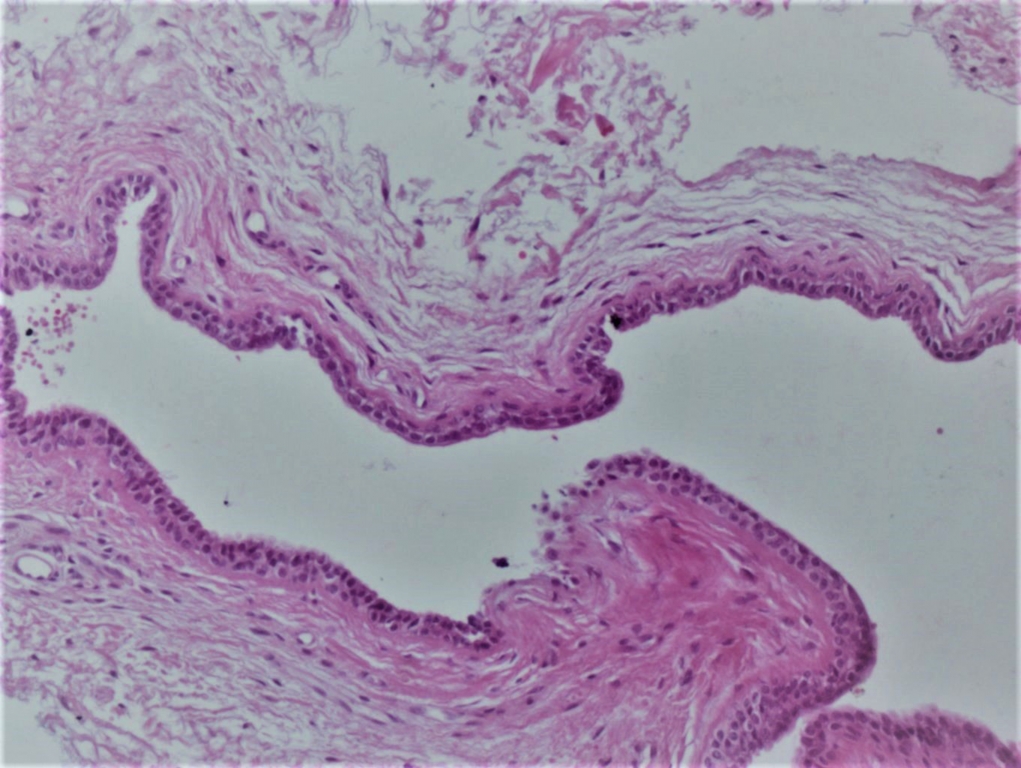
AbstractApocrine hidrocystomas are cystic bening tumors of the skin arising from secretory component of the apocrine sweat glands and usually occur solitary in the head and neck region especially around the eye, near the medial canthus. External ear involvement is very rare. These lesions may be translucent or colored. In this article, 43-years old female patient with slowly developing dark brown colored lesion on left anti-helix of the auricle is presented. Lesion was excised with the suspicion of melanotic lesion. Histopathologic analysis was reported as apocrine hidrocystoma. Although apocrine hidrocystomas are benign, they should be differ from melanotic malign lesions because some of them are colored. Complete excision and primarily closure of the skin usually sufficient for the treatment.IntroductionThere are two types of sweat gland on human body as eccrine and apocrine. Apocrine sweat glands in axillary and groin region also known as odoriferous sweat glands. And also, modified apocrine sweat glands locate at external ear canal, free margins of the eyelids and mammary glands of the breast [1]. Aprocrine hidrocystomas (AH) or cystadenomas are cystic bening tumors of the skin arising from secretory component of the apocrine sweat glands [2,3]. AH usually occur solitary in the head and neck region especially around the eye, near the medial canthus [2,4]. This lesions may be translucent or colored [4]. In the differential diagnosis, keep in mind malignant or benign cystic lesions [5,6]. Herein, we present a case of AH located anti-helix of the auricle. Only a few AH cases located ear reported in the literature. Three of them arise from external auditory canal and the other 3 cases of them arise from auricle. To the our knowledge, our presented case is fourth case of AH of auricle. Case Report43-years old female patient with slowly developing left auricular colored lesion lasting 8-9 months admit to our department of ENT. On the physical examination, there is dark brown lesion in diameter 3x2 millimeter on her left auricula. Lesion located mid-portion of the anti-heliks. Lesion had smooth surface and borders. In the medical history, she took Paroxetine for 6 years. After dermatology consultation, excision was planned in suspicion of melanotic lesion. Lesion was excised with fish mouth incision under local anesthesia. During the incision, cystic lesion spontaneously drained and lost its color partially. Incision was closed with 5/0 prolene suture by primarily. Specimen was sent to pathology department. Histopathologic examination of paraffin sections of the specimen, stained with haematoxylin-eosin (Figure 1,2), revealed the presence of a cyst in the dermis lined by a two-layered columnar epithelium resting on a layer with spindle myoepithelial cells. Lesion was reported as apocrine hidrocystoma.
DiscussionSweat glands divided as eccrine and apocrine sweat glands. Eccrine sweat glands present throughout the body and serve a thermoregulatory function via evaporative heat loss. Apocrine sweat glands (odoriferous sweat glands) gain the function at puberty with the stimulation of sex hormones. They are located in the groin and axillary region with hair follicles. Wax-producing ceruminous glands of the external auditory canal, the Moll glands found at the free margins of the eyelids, and the mammary glands of the breast are the modified apocrine sweat glands [1]. AH are benign and slow growing tumors of apocrine sweat glands. They usually locate around the eye especially margins of the eyelid, near the medial canthus. There is no sex differences and lesions frequent in 30-70 ages. AH usually occurs asymptomatic, solitary, in 3-15 mm diameter, dome-shaped, clear and smooth surfaces, skin colored or blue-black, brown colored lesions. There is no relation between climate and humidty [2,4]. Some bening lesions; eccrine hidrocystomas, cystic lesions such as epidermal cysts, mucoid cysts, hemangioma and lymphangioma are considered differential diagnosis. Eccrine hidrocystomas are solitary or multiple, frequent in females, 1-6 mm in diameter, often locate periorbital and malar region but not eyelid margin and affected heat and humid weathers [4] . Malign melanoma and basal cell carcinoma are the malign tumors in the differential diagnosis because AH are colored lesions [4,6]. Our case is dark-brown colored, smooth surfaced and small lesion. For the differential diagnosis, histopathologic examination was needed. Anzai et al. reported location rates of AH: face (61%), scalp (12.6%), trunk (13.7%), and extremities (12%) in Japanese cases [7]. In the literature, ear localization of AH is very rare. To our knowledge, three cases located external auditory canal and three cases located auricle reported [8-13]. One of the auricular AH case related gouty tophi of the pinna [11]. Our case has no systemic disease such as gout. There is only paroxetine use for 6 years in history. But, we could not find relation between drugs and AH in the literature. AH are usually asymptomatic. Recurrent otitis externa and hearing loss may occur in cases with AH located external auditory canal [9]. Our case was asymptomatic but had suspicion of melanoma due to its color. Simple needle puncture, excision, laser treatment, cauterization, incision and drainage, topical atropine or scopolamine creams had used for the treatment in the literature [4,11]. Incision and drainage have high recurrence rate and cauterization has risk of scar and there is no final diagnosis in these methods. Treatment of choice is complete excision because of histopathologic examination and difference of malignant lesions [8-,9]. Complete excision and primarily closure of the skin usually sufficient for the treatment because AH usually in small diameter. In our case, flap or graft was not needed. In conclusion, AH benign tumors of the skin due to sweat glands and very rarely locate at the auricle. AH should be differ from melanotic malign lesions because some of them are colored. Complete excision is the usually sufficient for the treatment. Conflicts of Interest We declare that there is no any existing or potential conflicts of interests, including financial, consultant, and institutional, that might lead to potential bias or a conflict of interest. References
|
|||||||||
| Keywords : kulak , hidrokistoma , ter bezleri , deri | |||||||||



|