Abstract
The anatomy of the paranasal sinuses is remarkably variable and it has to be known the abnormal structures and anatomical differences in order to prevent unwanted aesthetic results while performing rhinoplasty. Pneumatization can occur in the sinonasal area or its immediate environment, especially in the middle turbinate. Even though sinus frontalis might show enlargement in the lateral and supraorbital directions as a complication, medial pneumatization is extremely rare. In this case, we encountered a cavity related with right frontal sinus while doing hump resection. This is the first report of anterior nazoseptal cell of the frontal sinus
Introduction
Paranasal sinus and nasal septal skeleton malformations are common disorders[1]. Pneumatization can occur in the sinonasal area or its immediate environment. Pneumatization of the middle turbinate is more frequent, with occurrence rates of 8-20% healthy people and 20-43.9% in patients with rhinosinusitis[2] . In contrast, pneumatization of the inferior nasal concha, crista galli, perpendicular plate and clivus is very rare [3]. Due to the increasingly widespread rhinoplasty operations in the world, the long-term effects of surgical changes in the appearance and function of the nose have become more complicated. The accurate evaluation of anatomical variations helps the surgeon developing a more realistic surgical plan. In addition, it is critical to know the abnormal structures and anatomical differences in order to prevent unwanted aesthetic results. A detailed knowledge of the anatomy of the nose is very important for a successful rhinoplasty.
Case Report
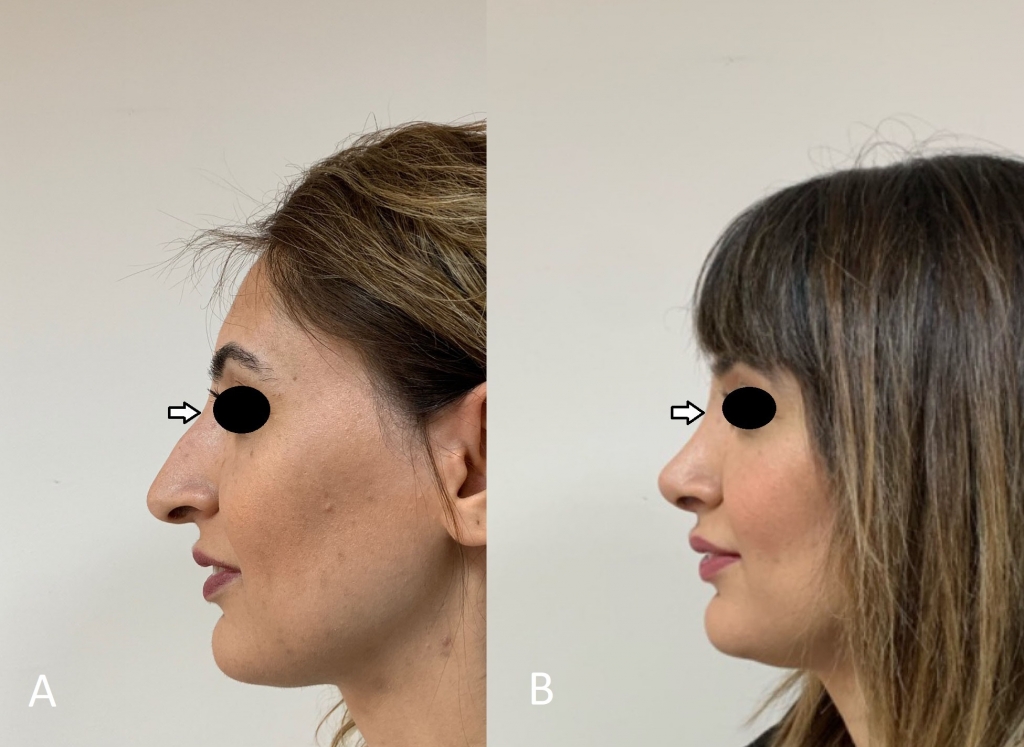
A 30-year-old female had difficulty breathing through the nose, in addition to a hump on the dorsum, and a low defined tip. The clinical examination of the patient who had not previously had nasal surgery, revealed the septum deviation to the right , the hump on the bone and cartilage dorsum, 75 degrees of nasolabial angle.
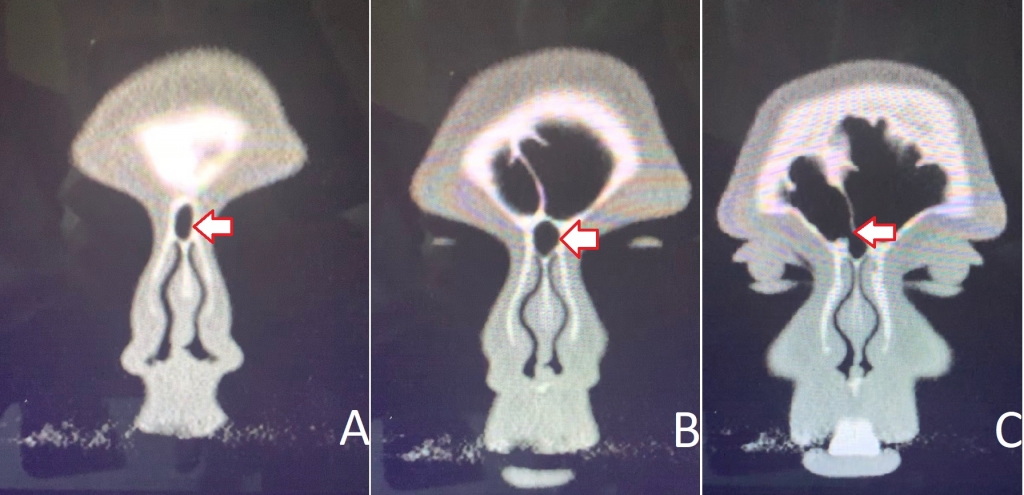
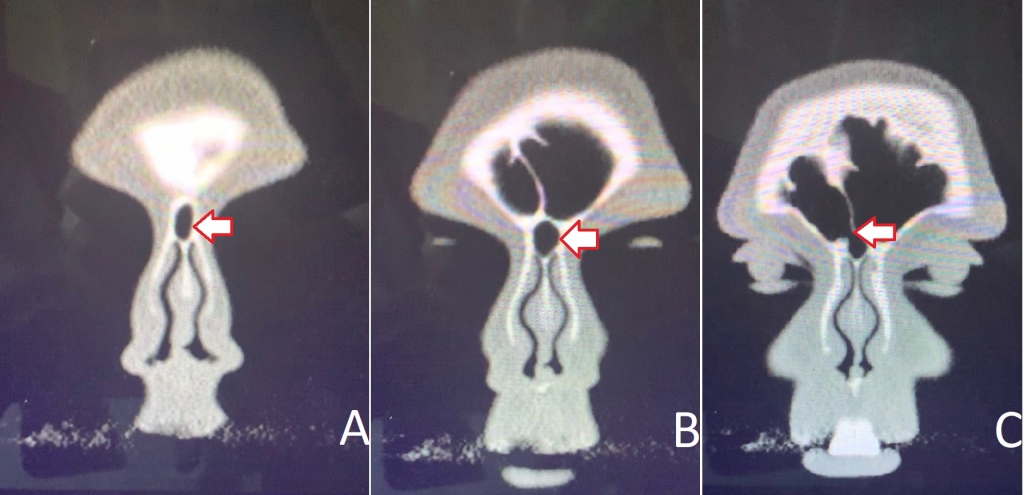
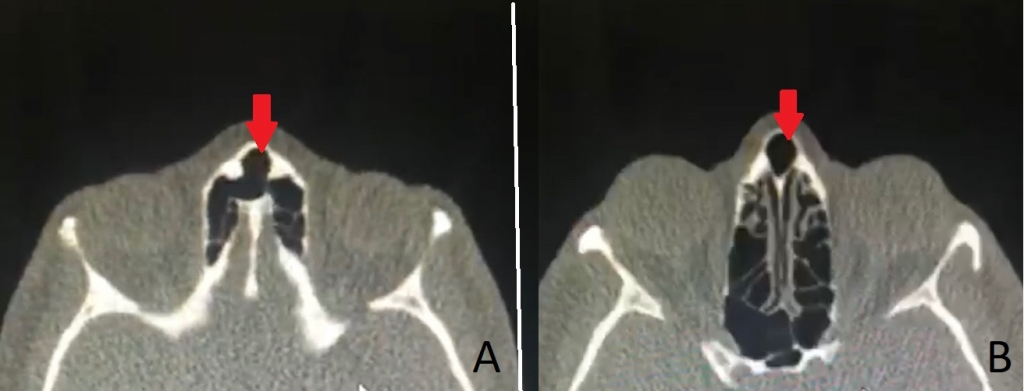
The patient was planned to perform rhinoplasty operation with open technique following radiological evaluation . In the paranasal tomography, 20x25 mm sized cell was present just below the nasal bone in the cranial of the k-connection point in the midline. The pneumotization had an osteum with 4 mm width and 3 mm length extending to the right frontal sinus (Figure 1 and 2).
Following the resection of hump intraoperatively, the relationship of the cell with the frontal sinus was seen more clearly through the endoscopic examination (Figure 3) The cell was observed as widening through the frontal sinus. After osteotomies, the hole was closed with an onlay cartilage graft and tried to prevent skin retraction. No deformity or infection was observed in the patient at the postoperative 12th month
Discussion
Paranasal sinuses and osteomeatal area are regions with quite a lot of anatomical variations[4]. Sinus frontalis usually consists of anterior ethmoid cells and reaches adult height at the age of 20. Sinus frontalis might show enlargement in the lateral and supraorbital directions, this provides convenience to the surgeon in operations with external approach. Pneumatization can occur in the sinonasal area or its immediate environment, i.e. the uncinate process, middle nasal concha, inferior nasal concha, crista galli, clivus. The perpendicular plate of the ethmoid bone, a major part of the bony skeleton of the nasal septum, is pneumatized in almost one third of the adult human population [5]. The septal pneumatization of frontal sinus has recently been described as frontal septal cell in a new system to clarify the pneumatization pattern of ethmoid and frontal sinuses introduced as the International Frontal Sinus Anatomy Classification (IFAC) [6] The cell originates from the region of the interfrontal sinus septum. and may occupy a part of the frontal drainage pathway. During all nasal surgeries, the surgeon should be ready to encounter in each case, considering the presence of these variations. Both anterior ethmoid and sinus frontalis- induced pneumatization may develop on the orbita ceiling . Thus sinuses are frontalier air accumulated behind the cavity often multiple (supernumerary) frontal sinus or recessus supraorbitalis termed Meloni et al.[7] encountered this variation at a rate of 18% in their radiological studies. In the literature there are only two cases have reported diagnosed as having mucocele originating from pneumatized of the anterior part of perpendicular plate. We should suggest that they were considered to be an independent pneumonization, since the authors did not mention the relationship of pneumotization to the frontal sinus[3,5] However, it is rare for the frontal sinus to extend from the full midline to the nasal bone, and our case is the first presentation that shows a junction of nasal bone and the frontal sinus in the literature .
Rhinoplasty is considered a high-risk operation, primarily due to the limited predictability of the aesthetic result. The structures that make up the nose are bones, cartilage, mucous membranes, skin, fat, fascia, muscles, nerves, veins, perichondrium and periosteum . The reactions of these tissues are not always under the control of the surgeon. This must be kept in mind particularly for cartilage and bones, the main support structure of the nose. The knowledge of anatomy is sufficient to minimize the complications.
We observed a large pneumotization extending to the frontal sinus after hump resection in rhinoplasty . When we search the literature, this is the first variation seen in rhinoplasty operations, cadavery and tomography scannings.[8]. Our treatment choice for bone defects was onlay cartilage grefting to prevent intranasal complications such as open roof syndrome, retraction, cosmetics and sinusitis . No complication was observed in the following year after the operation . We believe that this technique is ideal for fixing the dorsal defect in rhinoplasty.
References
- Sanchez Fernandez JM, Anta Escuredo JA, Sanchez Del Rey A, Santaolalla Montoya F (2000) Morphometric study of the paranasal sinuses in normal and pathological conditions. Acta oto-laryngologica 120 (2):273-278. doi:10.1080/000164800750001080
- Koo SK, Moon JS, Jung SH, Mun MJ (2018) A case of bilateral inferior concha bullosa connecting to maxillary sinus. Brazilian journal of otorhinolaryngology 84:526-528
- Wang RG, Zou YH, Han DY, Zhang W (2003) [Pneumatization of perpendicular plate of the ethmoid bone and mucocele]. Zhonghua er bi yan hou ke za zhi 38 (4):279-281
- Stokovic N, Trkulja V, Cukovic-Bagic I, Lauc T, Grgurevic L (2018) Anatomical variations of the frontal sinus and its relationship with the orbital cavity. Clinical anatomy (New York, NY) 31 (4):576-582. doi:10.1002/ca.22999
- Lei L, Wang R, Han D (2004) Pneumatization of perpendicular plate of the ethmoid bone and nasal septal mucocele. Acta oto-laryngologica 124 (2):221-222. doi:10.1080/00016480310015849
- Wormald PJ, Hoseman W, Callejas C, Weber RK, Kennedy DW, Citardi MJ, Senior BA, Smith TL, Hwang PH, Orlandi RR, Kaschke O, Siow JK, Szczygielski K, Goessler U, Khan M, Bernal-Sprekelsen M, Kuehnel T, Psaltis A (2016) The International Frontal Sinus Anatomy Classification (IFAC) and Classification of the Extent of Endoscopic Frontal Sinus Surgery (EFSS). International forum of allergy & rhinology 6 (7):677-696. doi:10.1002/alr.21738
- Meloni F, Stomeo F, Bozzo C, Dal Fiume R, Fancello B (1997) Computerised tomography evaluation of the frontal recess in inflammatory diseases of the frontal sinus: standardisation of a new technique. Rhinology 35 (1):28-32
- Harsha BC (2009) Complications of rhinoplasty. Oral and maxillofacial surgery clinics of North America 21 (1):81-89, vi. doi:10.1016/j.coms.2008.10.005
|