

Authors
|
|||||
AbstractSchwannomas are benign nerve sheath soft tissue tumors. These tumors are diagnosed histopathologically. Schwannomas typically show Antoni A or B cell structures. Although approximately 25-45 % of all schwannomas have been reported in the head and neck region, involvement of the lip philtrum is extremely rare. The authors report a case of schwannoma located on the upper lip philtrum of a 21-year-old male patient.IntroductionSchwannomas are benign encapsulated nerve sheath neoplasms, originating from the Schwann cell of the neural sheath. Schwannomas can arise almost anywhere, although the most common locations are the head and neck region. Approximately 25% to 45% of extracranial schwannomas present in the head and neck region. Schwannomas originate in the cranial, sympathetic, or peripheral nerves [1,2]. Schwannomas are the most common tumor of the peripheral nerve. Though schwannoma occurs as a solitary neurogenic tumor in the skin, schwannoma in the upper lip is very rare [3]. Case ReportA 21-year-old Turkish man presented with a 1-year history of a slowly enlarging and painless mass on the upper lip philtrum. His medical history was unremarkable. Physical examination revealed an approximately 10x10 mm nodulary mass extending from the midline philtrum to superior of the upper lip. The anterior surface of the swelling was hyperemic (Figure 1A,B). There was no evidence of cervical lymphadenopathy.
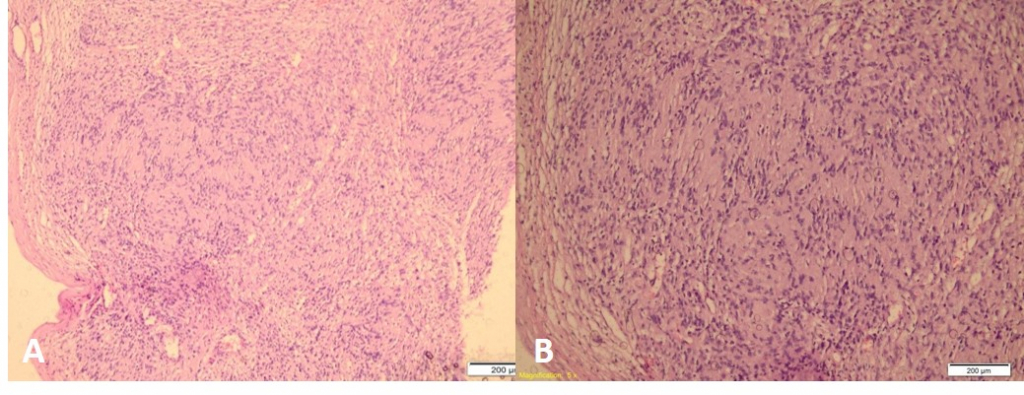
The mas was removed by excisional biopsy with local anesthesia and sent for microscopic examination. Microscopic examination of the solid mass showed Antoni type A tissue, that is, compact spindle cells arranged partly in short bundles or a fascicular pattern showing nuclear palisading and Verocay bodies. Areas of low cellularity termed Antoni B were also seen (Figure 2 A,B). Considering the microscopic features, final diagnosis of benign schwannoma was given. One year after resection, the patient had no evidence of residual or recurrent disease.
DiscussionSchwannoma is a rare benign tumor of the nerve sheath originating from Schwann cells. About 25–45 % of all schwannomas occur in the head and neck region. It is reported that about 20–58 % of head and neck schwannomas arise in the oral cavity and about 4% arise in the sinonasal region [2,4]. A systematic Pubmed literature review was conducted to include 25 cases of patients with schwannoma of the upper or lower lips. Most of patients presented with a single, painless, well-encapsulated nodule on the lip [5-10]. Head and neck schwannomas are not associated with sex preponderance, and although they can occur between the ages of childhood and very elderly, they are most commonly present at the age of 20–50 years [1]. Most of head and neck schwannomas present as a solitary, slowly growing, capsulated mass. Multiple schwannomas can be considered as part of the neurofibromatosis [1] . Clinical symptoms of extracranial schwannomas depend on tumor location, size and the nerve of origin. In the extracranial head and neck schwannomas, there are no specific symptoms or signs associated with masses, and most patients present with an asymptomatic palpable solitary mass [11].In our case, the symptom was painless swelling of the upper lip philtrum. Computed tomography (CT) and magnetic resonance imaging (MRI) have low sensitivity suggest the possibility of extracranial head and neck schwannomas in 35.7 and 33.3 %, respectively [12]. The complete surgical resection of the mass is the treatment of choice. Definitive diagnosis can only be confirmed by postoperative histopathologic examination. Histologically, the characteristic feature of a schwannoma is the pattern of Antoni A and Antoni B areas. Antoni A areas which contain tightly-organized nuclear palisades called Verocay bodies. Antoni B areas are less cellular and form no distinctive patterns. Immunohistochemistry staining plays an important role in accurate diagnosis. The positive stain with S-100 is specific to Schwann cells and is one of the histologic criteria used for diagnosis of schwannoma [2]. The differential diagnosis of extracranial and cutaneous schwannomas may be challenging due to the heterogeneity of clinical signs and the nerves of origin, as well as their size and localization. Other benign tumors, such as myoepithelioma, neurothekeoma, neurofibroma, solitary fibrous tumor, fibrous histiocytoma, leiomyoma, dermatofibrosarcoma protuberans, malignant primary tumors or metastatic masses, such as leiomyosarcoma ,malignant peripheral nerve sheath tumor, synovial sarcoma, melanoma, and metastatic disease, including carcinomas may mimic schwannomas [13]. In concusion, Schwannoma presenting as a nodulary mass in the upper lip philtrum is a rare phenomena however, it should be kept in the differential diagnosis with the cases of swelling in the upper lip philtrum. References
|
|||||
| Keywords : Schwannoma , filtrum , kitle | |||||


|