

Authors
|
|||||||||||||
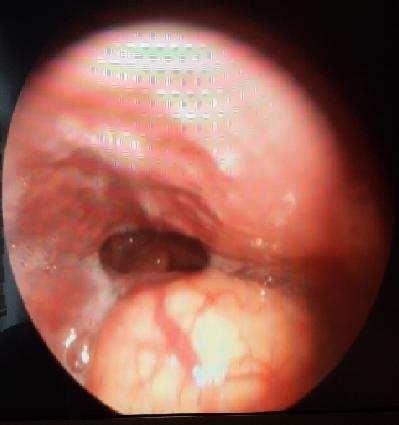
AbstractVallecular cysts are usually retention cysts of the minor salivary glands. Common site of occurence is lingual surface of epiglottis. Epiglottic mucous retentions, also known as vallecular cysts or base of tongue cysts. Small vallecular cysts are asymptomatic. These are may present different symptoms. In this latter, we describe the evaluation and treatment of a 60 year old man who presented with dysphagia and dispnea caused by large vallecular cysts.IntroductionLaryngeal cysts constitute approximate %5 of benign laryngeal lesions [1]. The lingual surface of the epiglottis is the commenest site [2]. These cysts have been classified as ductal cysts, retention cysts and lymphoepithelial cysts. These are caused by inflammation, irritation, or trauma [3]. Laryngeal cysts are rare entities with sporadic occurence and their prevalence and incidence are not precisely known. Epiglottic mucous retentions, also known as vallecular cysts or base of tongue cysts, are ductal cysts resulting from obstruction and retention of mucus in the collecting ducts of the submucosal glands located at the base of tongue [4]. Vallecular cysts are usually considered self-limiting lesions of the larynx, but in early infancy, this entity may be associated with severe airway obstruction and feeding difficulties [5-7]. In adults, vallecular cysts are most often asymptomatic and discovered on routine laryngoscopy or during induction of anesthesia. These cysts may present foreign body sensation in throat, dysphagia, dyspnea, voice change, and snoring [3]. We present a patient with large vallecular cyst who had complaints of foreign body sensation and pain in his throat during two years and applied many time to doctors due to his complaints. Case ReportA 60 year old man who presented with change voice, dyspnea, dysphagia and a lump in his throat for two years. He have not any other systemic disease. He had previously been treated with an antiinflamatuar and antibiotics bias his symptoms for upper airway infection. His otolaryngologycal examination was normal. But fibroscopic examination showed a large vallecular cyst (Figure 1).
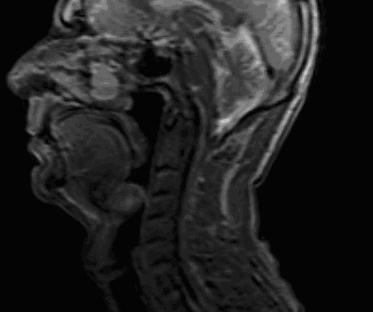
A computerized tomographic (CT) scan of the neck demonstrated a low density mass at epiglottis and vallecula (Figure 2). A magnetic rezolution (MR) scan of the neck a large hyper-intensity cyst between base of tongue and epiglottis (Figure 3).
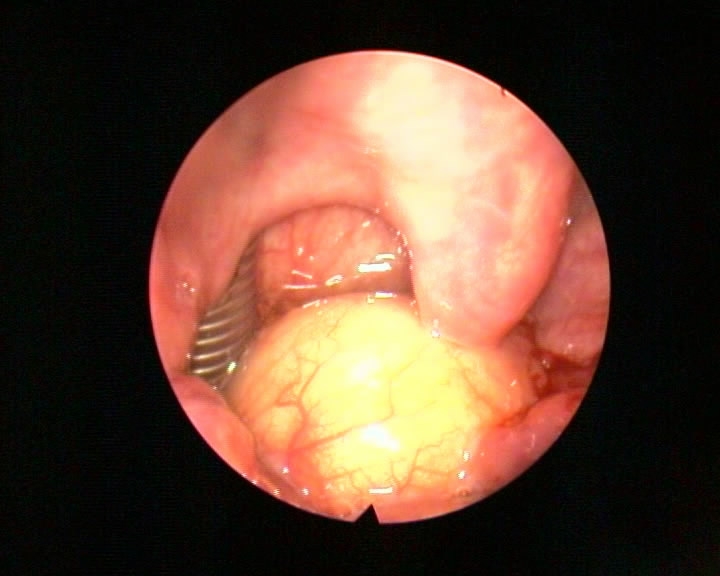
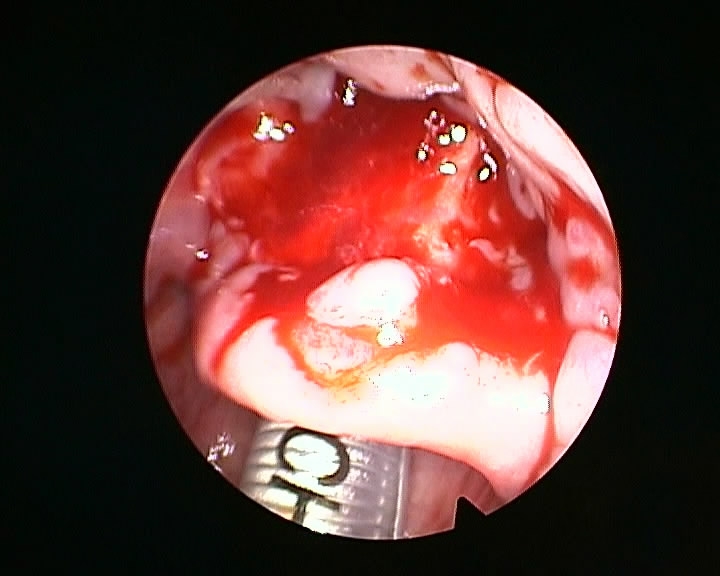
On the day of surgery, the patient was reassessed and particular attention was paid to his airway. The view of oropharyngeal structures was evaluated as Mallampati class 2. Based on the assesment and discussion with the anaesthetist. As patients with vallecular cyst have the potential for a difficult airway, in addition to tracheostomy and other difficult airway equipment, an otorhinolaryngology specialist was made available during anesthesia induction and tracheal intubation. Large-bore rigid suction catheters were also made immediately available in case of cyst rupture and bleeding. Under nasotracheal intubation with general anaestaesia (Figure 4), direct laryngoscopy and decompresion of the cyst with a long laryngeal needle were performed. Then, the cyst edge visualized and cyst was marsupialized (Figure 5).
Histopathological examination of the excised material confirmed a vallecular cyst. No problem arose during the course of anaesthesia, surgical intervention and the postoperastive period, and the patient was discharged on the third postoperative day. Postoperative 10th day, the patient’s examination was normal (Figure 6).
DiscussionLaryngeal cysts are rare, the first reported case was published by Abercrombie J in 1881 [8]. Vallecular cysts are retention cysts of the minor salivary glands in the vallecula and base of tongue. Obstruction of the mucous glands leads to cyst formation and continued secretion leads to a corresponding increse in size of the cyst. Vallecular cysts accounts for 10,5% to 20,1% of all laryngeal cysts [9]. The most common location of epiglottic cyst is lingual surface of the epiglottis. DeSanto et al. reviewed 238 cases of laryngeal cysts over a period of 10 years and found that 134(52%) were arising from the epiglottis [4]. The first classification was made by Myerson who divided of this cysts [10]. But the most popular one was postulated by DeSanto as ductal(75%) and saccular(25%) types [4]. Epiglottic cysts and vallecular cyst were attiributed to the ductal type and are caused by obstruction of the submucous duct. Epiglottic cysts are spesifically defined as cysts occuring at the lingual epiglottis. In adults, vallecular cyst are more common but less dangerous. Most adult epiglottic cysts are detected in the 6[th] decade of life, and the majority of cysts occur in men [3,6,11]. Presenting symptoms of epiglottic cysts vary with cyst size, age of the patient, as well as extension into the airway. Approximately two-thirds of vallecular cysts are asymptomatic and are diagnosed incidentally on routine laryngeal examination [3]. The incidence of vallecular cysts on laryngoscopy has been reported as 1 in 1250 to 1 in 4200, but their prevalance and incidence are not precisely known [12]. DeSanto at al. [4] stated that two separate clinical forms of vallecular cysts, with different pathogenesis and symptomatology. Majority of adult patients presenting with vallecular cysts may cause dysphagia and voice change . In ınfants and children it may also present with aero-digestive tract obstruction and stridor [6,13,14]. The differential diagnosis include internal thyroglossal duct cysts, dermoid cyts, lingual thyroid, teratomas, lymphangiomas and haemangiomas [15]. Bae et al. stated that a vallecular cyst in a patient with deep neck infection which cause difficult airway management [16]. Vallecular cysts can cause extreme problems in securing the airway. Meticulous airway assessment and contingency planning are mandatory, as with any difficult airway scenario. Close attention to logistics and the immediate availability of an otolaryngologist is vital [17]. Options for the treatment of vallecular cysts include wait and see, cyst aspiration, marsupialization , surgical debulking, microdebrider marsupialization, and laser excision [6,13,18-21]. In the case described here, the patient’s large vallecular cysts which caused dysphagia, and hot patoto voice. Vallecular cysts factor into the differential diagnosis of this symptoms. Managing vallecular cysts with direct laryngoscopy and excision may lead to resolution of symptoms. Conclusion In adults, vallecular cysts are most often asymptomatic and discovered on routine laryngoscopy or during induction of anesthesia. However, vallecular cysts may lead to dysphagia, voice change, dyspnea and globus. In evaluating this symptoms, the presence of a vallecular cyst should be considered. The patients with the complaints of foreign body sensation, odynophagia and pain throat should be performed laryngeal endoscopic examination and laryngeal cysts should be considered in diferantial diagnosis. Nasotracheal intubation is usefull in patients with vallecular cyst during the operation. References
|
|||||||||||||
| Keywords : Vallekula , büyük , Epiglot , Kist | |||||||||||||



|