

Authors
|
|||||||||||
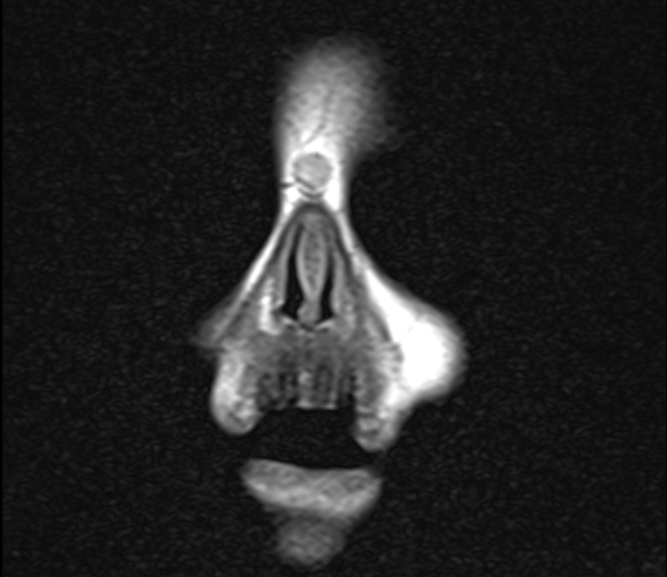
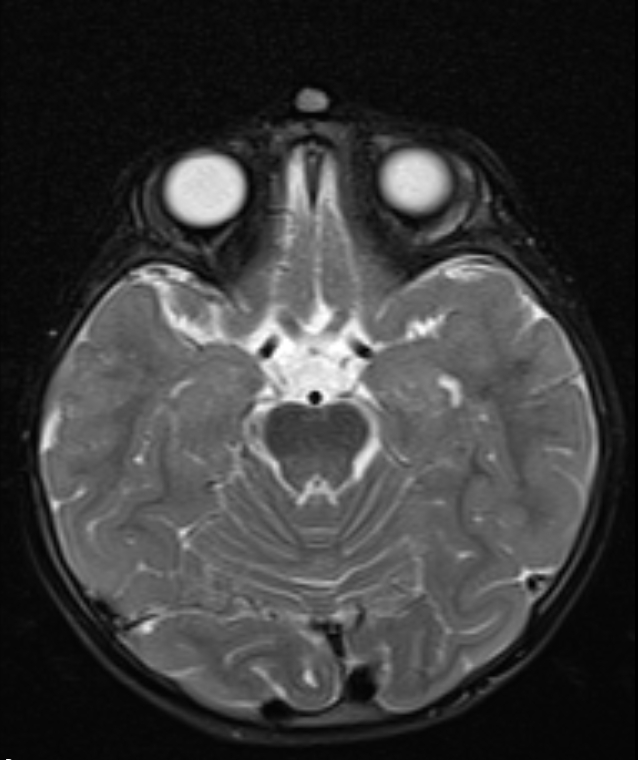
AbstractNasal dermoids usually present with a slow growing midline nasal mass and surgical excision is the recommended treatment because of their high risk of intracranial infection. We present the case of a superficial nasal dermoid cyst with a diameter of 1.2 cm in a 2-year-old boy and was successfully resected endoscopically with closed rhinoplasty approach via intercartilaginous incision. This is a rare case in which an extradural nasal dermoid cyst was resected endoscopically via closed rhinoplasty approach. Excellent cosmetic and surgical outcomes might be achieved by closed rhinoplasty approach in superficial, uncomplicated, extracranial dermoid cysts.IntroductionNasal dermoid cysts are rare congenital malformations with an incidence of 1/20,000-1/40,000 and the most common type of nasofrontal midline abnormality [1]. They usually present as a slow-growing midline nasal mass at birth, or they can manifest at any age. In some cases, they might be complicated with fistulas and sebaceous discharge, and a needle-like orifice with hair protrusion could be signs of nasal dermoid cysts [2]. In a current classification, there are four types of nasal dermoid; superficial, intraosseous, intracranial extradural, and intracranial intradural [3]. MRI is crucial for confirming the diagnosis, to determine the presence of a tract and intracranial involvement. CT could be complementary to evaluate nasal bone and the extent of intracranial involvement [3]. Surgical treatment is recommended because of cosmetic concerns, risk of intracranial infection, and susceptibility to enlargement[4]. Various surgical approaches for nasal dermoid cysts have been described including vertical nasal, transverse nasal, gull wing, bicoronal flap with frontonasal osteotomy, medial canthal (Lynch–Howarth), and external rhinoplasty approaches [5-7]. Excision of a nasal dermoid cyst without intracranial extension is the most preferred method. Endoscopy is usually used in cases with intracranial extension or skull base defects [4]. In this case report, a superficial nasal dermoid cyst with a diameter of 1.2 cm in a 2-year-old boy was successfully resected endoscopically with a closed rhinoplasty approach via the intercartilaginous incision. We presented the case with a clinical presentation, radiological images and a short surgical video. This is a rare case in which an extradural nasal dermoid cyst was resected endoscopically with a closed rhinoplasty approach. Case ReportParental consent was obtained for the publication of this case report. A 2-year-old boy came to our department complaining of painless swelling in the midline of the nose by his family.
The senior author experienced in closed rhinoplasty and endoscopic endonasal surgery carried out the surgical procedure. A left-sided intercartilaginous incision was made. The nasal dorsum was reached through the upper lateral cartilage. The nasal skin was retracted, and a good view was obtained with the 0̊endoscope. Dissection was completed in the supra perichondrial and supraperiosteal planes up to the radix and glabella. The procerus muscle fibers were then gently dissected and the cyst was exposed. A sharp elevator separated The cyst from the surrounding soft tissue and muscle fibers. The cyst was retracted upwards, and its base was evaluated. The cyst without bone erosion and intracranial extension was excised completely
DiscussionNasal dermoid usually present as a midline nasal mass and may be complicated with a sinus opening and discharge of sebaceous material, and recurrent infection. Nasal dermoid may be challenging to excise. To prevent recurrence, surgical access should allow complete excision in all circumstances. However, surgical access should be balanced against cosmetic results [8]. The conventional midline nasal and modified Lynch-Howarth incisions are long-established approaches. They both enable good exposure and, thus, straightforward dissection and resection. However, they both result in significant and obvious facial scarring, which may progress with age [9,10]. The external rhinoplasty approach offers excellent access to the nasal dorsum, facilitating gross resection of dermoid. However, the procedure causes a facial scar at the lower border of the nasal septum, not visible to the casual gaze [7]. In this case report, we performed endoscopic resection of a nasal dermoid cyst via the intercartilaginous incision. Compared to the other methods, this approach promises an excellent cosmetic result with a successful surgical outcome. This approach offers successful surgical outcomes,, with no skin incision, scarring, dressing, or short hospital stay. Also, our technique might be challenging in very large sizes, deeply located, complicated, and intracranial nasal dermoid. In a retrospective study by Hartley et al., dermoid cysts were located in the nasoglabellar region in 91 of 103 patients, and 90% were located extradural. Visible sinuses were observed in 66 out of 103 patients. All patients underwent surgery. Surgical and radiological concordance was 87%. Of 103 patients, 56 were treated with excision and direct closure, 37 with open rhinoplasty approach, 7 with bicoronal excision and craniotomy, and 3 with small window craniotomy [3]. In the study of Bradley et al. 61% of nasal dermoids were superficial, 16% extended to nasal cartilage, and 10% extended to nasal bone [11]. Since 60%-90% of nasal dermoids are classified as superficial, if there is no skin infection and fistulization, surgical procedure can be performed with endoscopic closed rhinoplasty. If there is an intracranial extension, most of them can also be treated with the endoscopic endonasal approach. Manickavasagam et al. described a novel method to excise an extracranial dermoid cyst in a 2-year of a child via scalp incision. They resected a dermoid cyst with a diameter of 1 cm endoscopically, without any face incision [7]. In an observational study of Ni et al., all 11 patients with extracranial nasal dermoid cysts were operated on with midface incisions. Seven of these patients had superficial nasal dermoid cysts ranging in size from 5-10 mm [12]. It is clear that endoscopic resection through the intercartilaginous incision could have successful outcomes and excellent cosmetic results, especially in superficial cysts of 1.5 cm or smaller in size. As these patients are usually operated on during infancy and early childhood, a scar on the midface will affect them for their entire life. Although endoscopic resections without face incision may not be applied in all cases due to technical difficulties but may provide successful outcomes and excellent cosmetic results in small, well-circumscribed, uncomplicated dermoid cysts. ConclusionIn this case report, a 1.2 cm diameter superficial nasal dermoid cyst was successfully resected endoscopically via intercartilaginous incision in a 2-year-old child. Excellent cosmetic results with successful surgical outcomes might be achieved by closed rhinoplasty approach in superficial located, well-circumscribed, uncomplicated, extracranial dermoid cysts. References
|
|||||||||||
| Keywords : dermoid kist , endoskopi , rinoplasti | |||||||||||




|