

Authors
Medipol Üniversitesi
Medipol Üniversitesi
Medipol Üniversitesi
Medipol Üniversitesi
|
|||||||
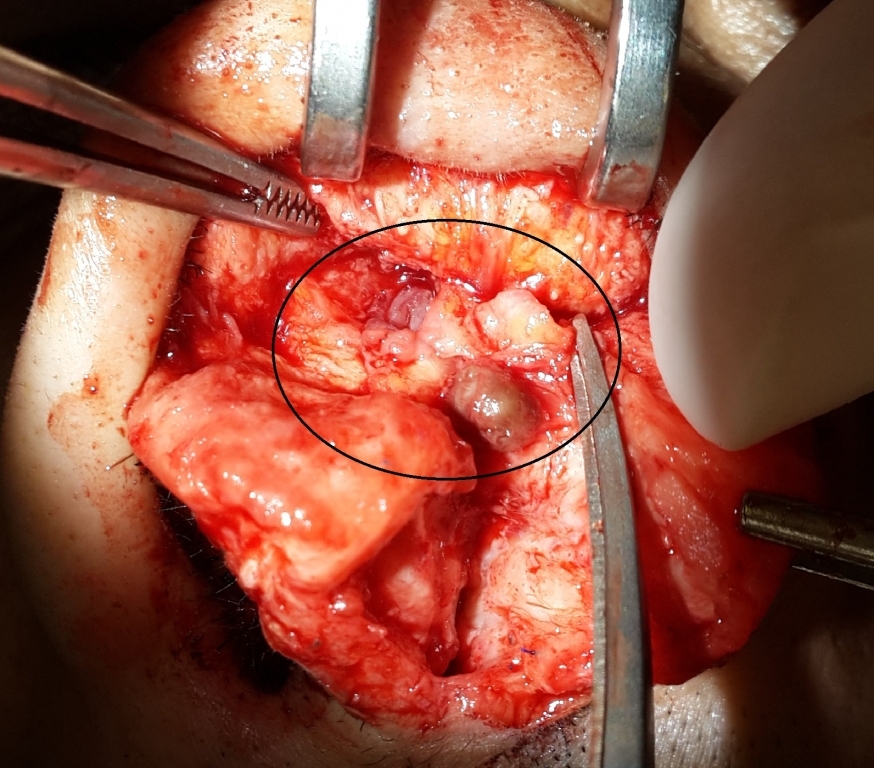
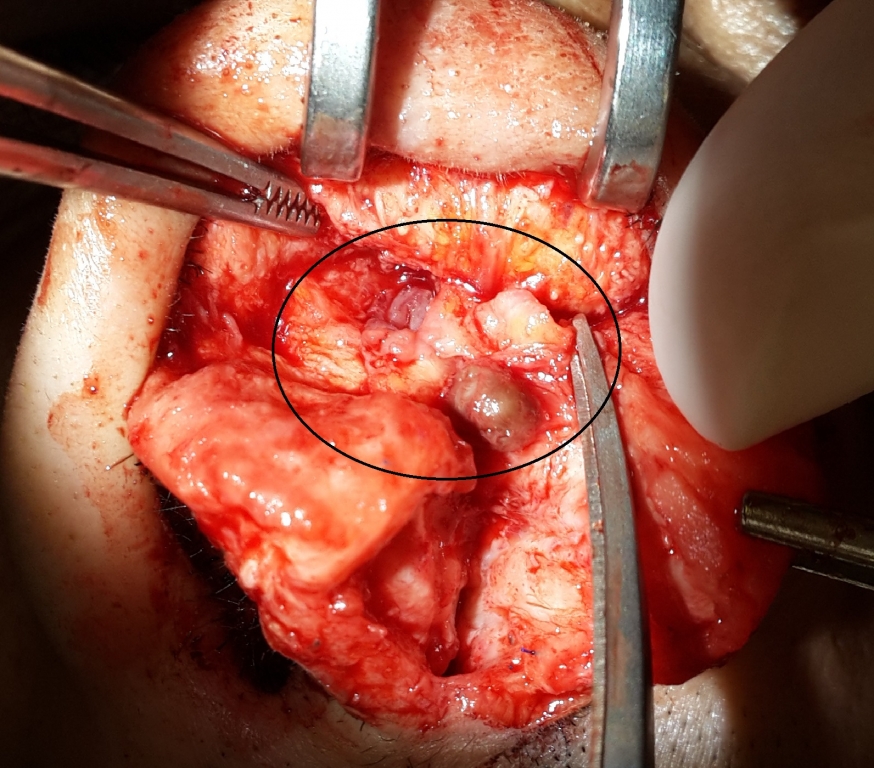
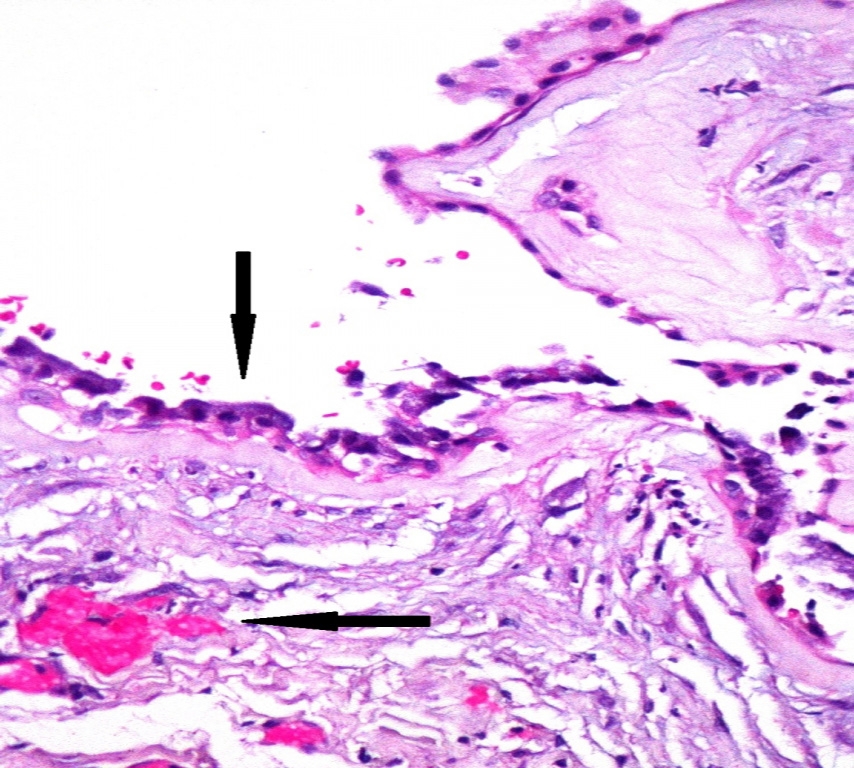
AbstractThe development of post-rhinoplasty nasal dorsal irregularities due to bone or cartilaginous bossae is a common complication; whereas, formation of cysts is a rare event. The patient presented here is a 34-year-old male patient who underwent a rhinoplasty surgery two times previously and had an irregularity on nasal dorsum. In his physical examination, synechia was present in the bilateral nasal cavity. Nasal passage bilateral was obstructed especially in the left side. Depression was present in the radix region of nasal dorsum. A mass with a smooth surface extending from the rhinion area in supratip region was observed. The cyst was removed as a whole together with its wall. Pathology result of the mass removed from the nasal dorsum was found to be compatible with the mucocele.IntroductionThe development of post-rhinoplasty nasal dorsal irregularities due to bone or cartilaginous bossae is a common complication; whereas, formation of cysts is a rare event. Reviewing previously reported cases has revealed that mucous cysts are the most prevalent in the nasal dorsum. Other locations include the nasal tip, the medial canthus, and the paranasal area [1-3]. Probably, migration or incorporation of mucosal tissue (or bony or cartilaginous fragments not completely removed during primary surgery performed in the subcutaneous space) commonly accounts for cyst formation[4]. With regard to non-mucosal cysts of the subcutaneous area, a fully different pathophysiology, namely foreign body reaction, may be considered. Petrolatum jelly migrated from the packing material and foreign body reaction to alloimplants employed for augmentation has been reported to be possible causes[5]. The patient presented here is a 34-year-old male patient who underwent a rhinoplasty surgery two times previously and had an irregularity on nasal dorsum. Case ReportThe 34-year-old male patient applied with complaints of the difficulty in breathing through the nose and nasal deformity. In his history, he expressed that he had two rhinoplasty surgeries, the latest one of which was performed 2 years before. In his physical examination, synechia was present in the bilateral nasal cavity. Nasal passage bilateral was obstructed especially in the left side. Depression was present in the radix region of nasal dorsum. A swelling was distinguished in the supratip area (figure-1). Tip was low and columella collapsed because of the absence of a support cartilage in the septum. He had no pathology in his laboratory examinations. A surgery indication was specified for the patient in order to have him to breathe through his nose and to correct the significant nasal deformity. After a consent was taken from the patient due to the necessity of taking cartilage from his rib, the patient was referred to surgery. The surgery started under general anesthesia and a graft was taken from the 8[th] costal cartilage. Then, nasal dorsal skin was elevated by entering through midcolumellar incision. A mass with a smooth surface extending from the rhinion area in supratip region was observed (figure-2). At first, the mass gave the impression of a synthetic material applied in the previous surgery. When the mass was incised by using a scalpel, a mucoid material inside the mass was aspirated. The cyst was removed as a whole together with its wall. The operation was finalized after septum and dorsum reconstruction. Pathology result of the mass removed from the nasal dorsum was found to be compatible with the mucocele (figure-3). Then dorsal reconstruction and augmentation were performed (figure-4). No relapse was observed at the follow-up of the patient on the 6[th] post-op month.
DiscussionAccording to the literature, the different circumstances of the cases presented here suggest different pathways for formation of cysts. The most accepted theories about the etiology of mucous cysts after aesthetic rhinoplasty include the presence of ectopic free mucosal graft implantation during surgical treatment, herniation of mucosa through intranasal incision, improper clearing of mucous epithelial remnants, or bony and cartilage parts during the operation [6,7]. Other possible causes could be intrasurgical trauma and occlusion of sebaceous glands from scar tissue formation [8]. Inflammatory reaction to a foreign body has also previously been described as a possible cause [9]. In our case, it was more likely considered that there could be a mucosal implantation in the pathogenesis due to the location of the cyst. In this region, if the nasal mucosa under the cartilages are not elevated during the hump resection and cephalic resection and if its integrity is impaired, it may enlarge towards the nasal dorsum or may produce secretion. Or after the deep transition of the permanent sutures placed in the nasal dorsum and after the contact with the nasal mucosa, the possibility of the transition of epithelium and secretions in the nose to the nasal dorsum appears. Another possible mechanism is that the grafts placed in the nasal dorsum for augmentation purpose consist of mucosa islets. In such cases, cyst formation is possible because mucosal proliferation and secretion will continue. When treating nasal dorsal masses, one first has to exclude various nasal lesions not related to surgery: neoplastic lesions, benign processes, encephaloceles, gliomas, dermoids, osteomas, lipomas, granulomatous diseases (Wegener granulomatosis, sarcoidosis, and rhinoscleroma), and infections (fungus, syphilis, and tuberculosis) [10]. It was thought that irregularity and swelling before the surgery were associated with problems in skeleton of nasal dorsum caused by previous surgeries since our case had history of two previous rhinoplasty surgeries and no infection finding such as hyperemia on nasal dorsum. The treatment of such cysts encountered on the nasal dorsum is cyst excision and nasal dorsal reconstruction. In our case, after the cyst observed incidentally in the nasal dorsal region was excised together with its wall, dorsal augmentation was applied by costal cartilage graft. In conclusion, mucocele should be considered in differential diagnosis if a swelling is determined on the nasal dorsum in the patients who underwent rhinoplasty previously. In order to avoid such complication, we think that it is required to be sure that mucosal elevations are performed before the osteotomies, to be aware of mucosal contamination if any, to suture the mucosa with appropriate sutures in such a way to recover within their own media, be sure that the grafts placed in nasal dorsum do not contain any mucosa, to avoid from deep and permanent sutures that may relate the nasal cavity mucosa with the nasal dorsum soft tissue and to avoid from using materials that may cause foreign body reactions. References
Presented at11. Türk Rinoloji Kongresi'nde poster olarak sunuldu. |
|||||||
| Keywords : Mukosel , Rinoplasti , Nazal dorsum | |||||||

|