

Authors
|
|||||||
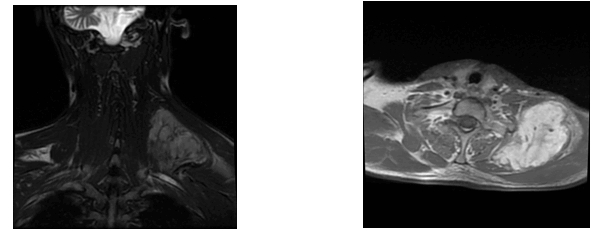
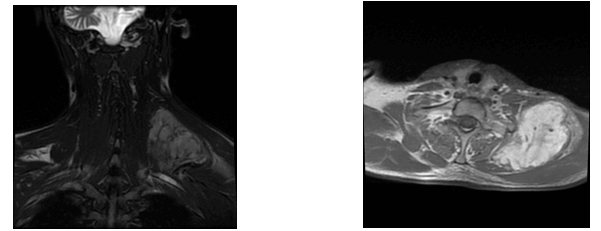
AbstractLeiomyoma is a benign soft tissue neoplasm originating from smooth muscles. While leiomyomas most frequently occur in the uterine myometrium (95%), they are also found in the skin (3%), gastrointestinal system (1.5%), and in less than 1% of cases in the head and neck region . The tumor generally appears in the 4th and 5th decades of life, more commonly in females, and typically presents as a slow-growing, asymptomatic lesion.The main treatment for leiomyoma is surgical resection, and recurrence is quite rare. In this case report, we present a rare case of a giant solid leiomyoma located in the supraclavicular region, which we evaluated clinically, histopathologically, and radiologically IntroductionLeiomyoma is a benign neoplasm arising from smooth muscle cells and is most commonly found in the uterus, skin, and gastrointestinal tract. However, due to the limited presence of smooth muscle tissue in the head and neck region, leiomyomas in this area are extremely rare, accounting for less than 1% of all cases. These tumors generally present as slow-growing, painless masses and are more frequently observed in middle-aged women. Histopathologically, leiomyomas consist of bundles of well-differentiated spindle cells with eosinophilic cytoplasm and show strong immunoreactivity for smooth muscle markers such as smooth muscle actin (SMA), desmin, and caldesmon. Based on histological features, leiomyomas are classified as solid leiomyoma, vascular leiomyoma (angioleiomyoma), and epithelioid leiomyoma. Although their pathogenesis remains unclear, theories suggest that they may originate from the vascular smooth muscle of small blood vessels or pluripotent mesenchymal cells. Surgical excision remains the mainstay of treatment, and recurrence is uncommon. In this report, we present a rare case of a giant solid leiomyoma located in the supraclavicular region, evaluated clinically, radiologically, and histopathologically. Case ReportA 33-year-old male presented to the Otorhinolaryngology Department of Antalya Training and Research Hospital with a complaint of swelling in the left supraclavicular region for six months, which had gradually increased in size. On physical examination, a firm, fixed, smooth-surfaced, tender mass approximately 7x5 cm in size was palpated in the left supraclavicular area. Neck ultrasound revealed a heterogeneous hypoechoic mass lesion originating from muscle tissue on the left lateral neck measuring 78x68x36 mm. MRI of the neck showed a mass lesion located posteriorly in the left supraclavicular region with a maximum size of 91x58 mm, hyperintense on T2-weighted images, and intensely enhanced after intravenous contrast administration (Figure 1). Fine-needle aspiration (FNA) biposy was and diagnosis of a benign spindle cell benign tumor was made.
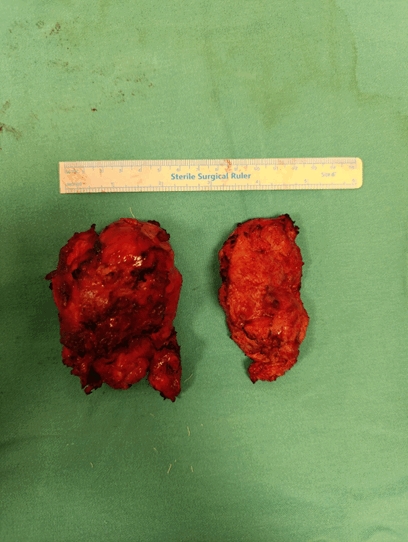
Under general anesthesia, a mass extending to the scapula was excised in two parts while preserving the phrenic nerve and brachial plexus (Figure 2). The larger mass measured 9x6x4.5 cm, and the smaller 8x4.5x4.5 cm.
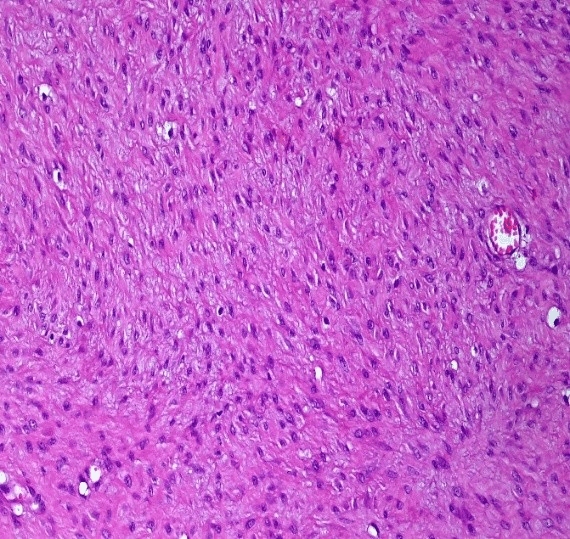
Histopathological examination confirmed the diagnosis of leiomyoma (Figure 3).
DiscussionA systematic approach and treatment plan should be followed for differential diagnosis of supraclavicular masses. Inflammatory events and benign lesions are more common in young adults, while malignancies are more likely in patients over 40. Our patient was under 40 years of age and had a benign lesion, leiomyoma. Leiomyomas are most commonly seen in the uterine myometrium (95%), followed by the skin (3%), gastrointestinal tract (1.5%), and less than 1% in the head and neck region [1]. Our case was particularly rare due to its supraclavicular location. Detailed patient history and physical examination are crucial for diagnosis. Conditions such as prior diseases, trauma history, and accompanying symptoms should be questioned. Physical exam should assess mass mobility, firmness, and presence of bruits. Systemic examination is essential, as many masses in this region are secondary findings. In our case, the mass was immobile with no bruits, and the patient had a trauma history but no known chronic diseases. Leiomyomas often contain calcifications and their clinical appearance is usually an asymptomatic, slowly growing mass [5]. However, in our case, the mass grew rapidly within 6 months. It can be challenging to distinguish leiomyoma from leiomyosarcoma preoperatively, and indeed in our case there was suspicion of invasion of the surrounding muscle tissue and scapula on preoperative imaging, but this suspicion was reduced when the FNA biopsy was reported as benign. Histologically, the tumor showed eosinophilic spindle cells, consistent with literature. Immunohistochemical staining was positive for SMA and calponin, and the Ki-67 index was <1%, also consistent with existing data. Proposed mechanisms for leiomyoma development include congenital origin, vascular abnormalities, infection, and estrogen involvement, although no consensus exists. Progesterone receptors have also been shown to be expressed in tumor cell nuclei, possibly explaining higher prevalence in females [6]. Although trauma is not usually involved in etiology, the mass developed after a trauma he experienced four years ago. Although FNA biopsy may be difficult due to calcification, we believe that this procedure may be the first choice to differentiate benign from malignant leiomyoma in the neck. ConclusionIn conclusion, we present a rare case of giant leiomyoma in the supraclavicular fossa. This case report emphasizes that leiomyoma should be considered as a differential diagnosis when investigating patients with a lateral neck mass. References
|
|||||||
| Keywords : leimiyom , supraklavikular kitle , düz kas | |||||||
|